

Whiplash is a non-medical term describing a variety of neck injuries caused by or related to a sudden distortion of the neck associated with the extension, although the exact injury mechanism is still unknown. The term "whiplash" is a colloquial language. "Cervical acceleration-deceleration" (CAD) describes the mechanism of injury, while the term "whiplash associated disorders" (WAD) describes residual symptoms and symptoms of injury.
Whiplash is generally associated with motor vehicle accidents, usually when the vehicle has been hit behind; However, injuries can be maintained in many other ways, including headbanging, bungee jumping and falling. This is one of the most frequently claimed injuries to vehicle insurance policies. In the United Kingdom, 430,000 people made insurance claims for whiplash in 2007, accounting for 14% of each driver's premium.
Prior to the invention of cars, whiplash injuries were called "railroads of the spine" as they were largely recorded with respect to train collisions. The first case of severe neck pain arising from a train collision was documented around 1919. The number of whiplash injuries has increased sharply due to a rear-end vehicle collision. Given the various symptoms associated with a whiplash injury, the Quebec Task Force on Match-Whiplash Matching coined the term 'Whiplash-Associated Disorders'.
Video Whiplash (medicine)
Signs and symptoms
Symptoms reported by the patient include: pain and pain in the neck and back, pain referred to the shoulder, sensory disturbances (such as pins and needles) to the arms and legs, and headaches. Symptoms can appear immediately after injury, but often do not feel until many days afterwards. Whiplash is usually confined to the spine. The most common areas of the spine affected by whiplash are the neck and middle of the spine. Pain "Neck" is very common between the shoulders and the neck. The "missing link" of whiplash may be toward or inside the shoulder and this will explain why neck therapy alone often does not provide lasting help.
Cognitive symptoms after a whiplash trauma, such as easily irritated or irritated, appear to be common and may be associated with a worse prognosis.
Maps Whiplash (medicine)
Cause
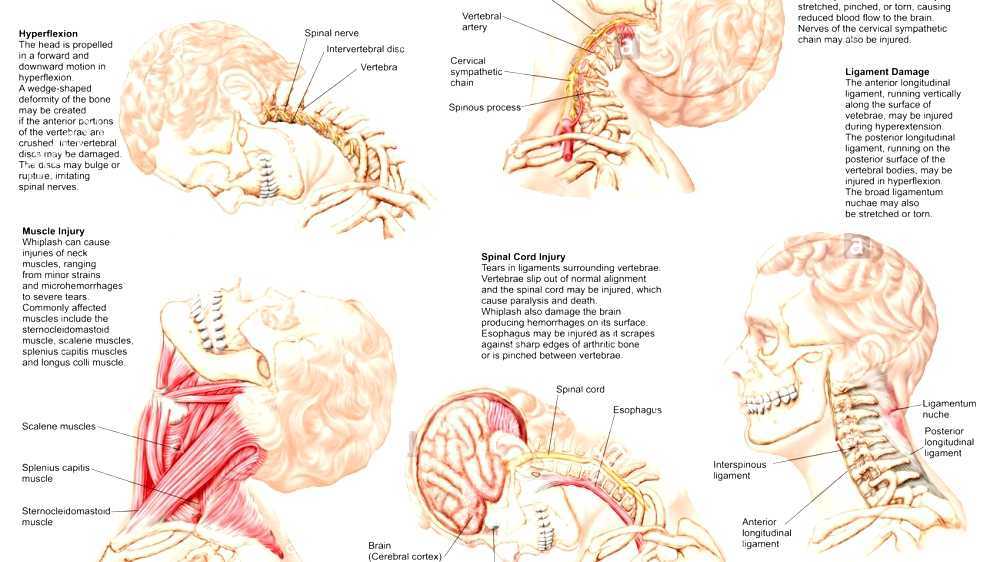
The exact injury mechanism that causes whiplash injury is unknown. A whiplash injury may be caused by the withdrawal of the impulse from the spine, especially the ligaments: the anterior longitudinal ligament that stretches or rips, when the head is locked forward and then back again causing a whiplash injury.
A whiplash injury from a car accident is called acceleration acceleration-slowing injury. The study of corpses has shown that as occupants of the car are struck from behind, the power of the rear seat suppresses thoracic spinal cyphosis, which provides axial load on the lumbar spine and cervical spine. This forces the cervical spine to transform into an S-shape in which the cervical spine is forced downwards into kyphosis while the upper cervical spine retains its lordosis. As the injury progresses, the entire cervical spine is finally hyper-extended.
Whiplash can be caused by any motion similar to a collision behind a motor vehicle, as may occur in roller coasters or other rides in amusement parks, sports injuries such as skiing accidents, other modes of transportation such as traveling aircraft, or from being beaten, kicked or shaken..
Whiplash-related disorders sometimes include cerebrum injuries. In severe cervical acceleration syndrome, a brain injury known as coup-coup coup d'etation occurs. A coup-counter coup coupe occurs when the brain is accelerated to the skull as the head and neck hyperextend, and then accelerated to the other side as the head and neck bounce to a hyperventative or neutral position.
"Experimental volunteer studies, low rear-speed collisions have shown the percentage of subjects to report short-lived symptoms",
From this type of research it has been concluded that whiplash symptoms may not always have pathological explanations (injuries). However, over the last decade, academic surgeons in Britain and the US have sought to solve puzzling puzzles. A 1000-case observational study, four years published in 2012, says that the "missing link" in a whiplash injury is a trapezius muscle that may be damaged through eccentric muscle contraction during the whiplash mechanism described above and below. Another study showed that "shneck pain" was in nearby supraspinatus muscles and this resulted from a seemingly asymptomatic form of shoulder impingement. Shoulder impingement is usually asymptomatic and the shoulder may be injured along with the neck in a motor vehicle accident. Whiplash because Recommended Shampoo Binding Syndrome was successfully treated by using conventional treatments for shoulder implosion including steroid and non steroidal anti-inflammatory, and by avoiding the overhead position of the shoulder throwing during the day and night. All of this work shows that historically and indeed currently whipping the patient's pain sources may be missed if it is outside the neck. Therefore pathology in whiplash may be missed and treatments are ineffective.
Overall it should be noted that especially in many Western countries, after a motor vehicle collision, those involved seek medical care for injury assessment and for the purposes of insurance documentation. Conversely, in many less wealthy countries, access to limited care and insurance may only be available to the rich. Against this backdrop, "whiplash syndrome" (ICD-10: S13.4) has been one of the main focuses of continuous and controversial scientific research since the 1950s because the worldwide incidence of such injuries varies considerably 16- 2000 per 100,000 population. and the final whiplash syndrome in this case varies between 18% and 40%. Thus, the important work of Schrader et al in The Lancet shows that the final whiplash syndrome following a motor vehicle collision is rare or not common in Lithuania, and Cassidy et al's conclusion in the New England Journal of Medicine > is that "the elimination of compensation for pain and suffering is associated with decreased incidence and improves the prognosis of whiplash injury". In addition, one should also mention an experimental study in 2001 in which participants were placed in stationary vehicles with blinds blocking their rear view, and exposed to rear-simulation collisions. Twenty percent of patients experience symptoms at 3 days, despite the fact that no collisions actually occur. From the evolving point of view of naturalistic Internet search engine analysis it has been shown in 2017 that the expectation of receiving compensation can affect the behavior of Internet searches in relation to whiplash injuries.

Mechanism
Whiplash can be described as a sudden tension in the muscles, bones and nerves in the neck. The neck is made up of seven vertebrae, which are referred to as cervical vertebrae. The first two cervical vertebrae, axis and atlas, are formed differently from the remaining five. Atlas and axis are responsible for skull movement from side to side (cervical rotation to the right and left); also moving forward and backward (cervical flexion and extension). Excessive and excessive flexibility can disrupt the vertebrae.
There are four phases that occur during "whiplash": Initial position (before collision), retraction, extension, and rebound. In the initial position there is no force on the neck that is stable due to inertia. Longitudinal anterior cruciate ligaments on whiplash can cause cervical instability. They explain that during the retraction phase that is when the actual "whiplash" occurs, there is an unusual loading of soft tissue. The next phase is the extension, the entire neck and head switch to the extension, and it is stopped or restricted by head restraints. The rebound phase occurs as a result of the mentioned phase.
During the phase of the spinal retraction forms the S-Shaped curve, and this is due to flexion in the upper plane and hyperextension at the bottom of the plane and this goes beyond the physiological limits of this phase, the injury occurring in the lower cervical vertebra. In the extension phase all cervical and head vertebrae are fully extended, but not beyond their physiological limits. Most of the injuries occur in C-5 and C-6.

Pathophysiology
While the time associated with a particular collision will vary, the following gives an example of the order of interaction of occupants and seats for a collision that lasts about 300 milliseconds.

Diagnosis
Diagnosis occurs through patient history, head and neck examination, X-rays to exclude fractures and may involve the use of medical imaging to determine if there are other injuries.
QuÃÆ' Â © bec Task Force
The QuÃÆ' Â © bec Task Force ( QTF ) has split whiplash related disturbances into five classes.
- Value 0: no neck pain, stiffness, or any physical signs of concern
- Level 1: complaints of pain, stiffness or neck pain but no physical signs recorded by the examining physician.
- Level 2: neck complaints and checking doctors found decreased range of motion and pain point in the neck.
- Level 3: neck complaints plus neurological signs such as decreased deep tendon reflexes, weakness and sensory deficits.
- Level 4: neck and fracture complaints or dislocations, or injury to the spinal cord.

Prevention
The focus of preventative measures to date is on car seat design, especially through the introduction of head restraints, which are often called headrests. This approach is potentially problematic given the underlying assumption that pure mechanical factors cause whiplash injury - an unproven theory. So far the effect of reducing injuries from head restraints appears to be low, about 5-10%, as car seats become more rigid to increase the lethargy of cars in high-speed rear collisions which in turn may increase the risk of whiplash injury in low-impact collisions. Improvements in the geometry of the car seat through better design and energy absorption may offer additional benefits. The active device moves the body in a collision to shift the load in the car seat.
Over the past 40 years, vehicle safety researchers have designed and collected information on the ability of head restraints to reduce injuries from rear-end collisions. As a result, various types of head restrictions have been developed by various manufacturers to protect their occupants from whiplash. Below is the definition of different types of head restraints.
Barrier head - refers to a device designed to limit the displacement of adult headaches with respect to the torso to reduce the risk of injury to the cervical vertebra in the event of a collision in the back. The most effective head barrier should allow backset motion less than 60 mm to prevent neck hyperextension during impact.
Integrated headguards or fixed headgear - refers to the head restraints formed by the top of the backrest, or unregulated head restraints and can not be removed from seat or vehicle structures except by means of tools or following removal part or total of the furniture of the chair ".
Adjustable head barrier - refers to head restraints capable of being positioned to fit the morphology of occupants sitting. The device can allow horizontal displacements, known as tilt adjustments, and/or vertical displacements, known as high adjustments.
Active head dismissal - refers to devices designed to automatically increase the position of head restraints and/or geometry in the event of a collision ".
Automatically adjust head restraints - refers to head restraints that automatically adjust the position of the headrest when the seat position is adjusted.
A major problem in the prevention of whiplash is the lack of proper adjustment of the seat security system by drivers and passengers. Studies have shown that a well designed and well-designed head buffer can prevent potentially adverse head-neck kinematics on rear collisions by limiting the differential motions of the head and torso. The main function of head restraints is to minimize relative rear and head back movements during the back collision. During a rear-end collision, the presence of an effective head restrain behind the occupants' head can limit the differential motion of the head and torso. Properly placed head control where a person can adequately protect his head, the possibility of head injury up to 35% during rear collision.
In contrast to well-adjusted headgear, studies show that there may be an increased risk of neck injury if the head restraint is not positioned correctly. More studies by manufacturers and car safety organizations are currently undergoing to examine the best way to reduce head and torso injuries during rear-end impacts with different geometries of head control and headrest systems.
In most passenger vehicles where manual adjustable head restraints are installed, proper use requires sufficient knowledge and awareness by occupants. While driving, the height of head restraints is very important in influencing the risk of injury. The barrier must be at least as high as the center of gravity of the head, or about 9 centimeters (3.5 inches) below the top of the head. The backset, or the distance behind the head, should be as small as possible. Backsets of more than 10 cm (about 4 inches) have been associated with increased symptoms of neck injury in crashes. In a sitting position, the minimum height of restraint should correspond to the top of the driver's ear or even higher. In addition, there should be a minimum distance between the back of the head and the point where it first encounters the restraint.
Because of the low public awareness of the consequences of incorrect placement of head restrictions, some passenger vehicle manufacturers have designed and implemented various devices into their models to protect their occupants.
Some of the current systems are:
- Mercedes-Benz A-Class Active Head Restraint (AHR),
- Saab (Responsible for active first head control), Opel, Ford, Nissan, Subaru, Hyundai, and Peugeot - Active Head Control (SAHR),
- Volvo and Jaguar - Whiplash Protection System/Whiplash Prevention System (WHIPS), and
- Toyota - Whiplash Injury Lessening (WIL).
Insurance Agencies for Highway Safety (IIHS) and other testing centers around the world have been involved in testing the effectiveness of head and seat restraint systems in laboratory conditions to assess their ability to prevent or reduce whiplash injuries. They have found that over 60% of new motor vehicles in the market have "good" head tightness. Various organizations have listed such vehicles

Management
Rehabilitation (eg physical therapy)
Symptoms remaining more than six months after trauma are labeled Whiplash syndrome. The primary goal with early rehabilitation is to reduce the risk of developing Whiplash syndrome. The initial rehabilitation for whiplash depends on the class category. This can be categorized as grade 0 painless to grade 4 with fractures or cervical bone dislocations. Grade 4 clearly needs to enter the hospital while the class 0-3 can be managed as an outpatient. The symptoms of a potential injury to the cervical spine may be debilitating, and pain is reported to be one of the greatest stressor events experienced in everyday life, so it is important to start an immediate rehabilitation to prevent future pain.
Current research supports that active mobilization rather than soft collars results in faster recovery in both short and long term perspectives. Furthermore, Schnabel and colleagues note that soft collars are not a suitable medium for rehabilitation, and the best way to recover is to include an active rehabilitation program that includes physical therapy exercises and postural modification. Another study found that patients who participated in active therapy soon after the injury increased neck mobilization with much less pain within four weeks when compared to patients using cervical collars.
Active treatment is a light repetitive exercise that works in the area to maintain normality. Basic information is also provided to teach patients that exercises as instructed will not cause damage to their necks. These exercises are done at home or under the care of a healthcare professional. When starting a rehabilitation regimen, it is important to start with a slow motion that includes cervical rotation to the pain threshold three to five times per day, flexion and extension of the shoulder joint by moving the arms up and down two to three times, and combining the shoulder increments. while inhaling and releasing his shoulders while breathing out. Soderlund and colleagues also recommend that this exercise should be done daily until the pain begins to disappear. Early mobilization is important to prevent chronic pain, but the pain experienced by this exercise can lead to psychological symptoms that can have a negative impact on recovery. Rosenfeld found that doing active exercises as often as once every hour for a month after the trauma reduced the need for sick leave three years after the trauma from 25% to 5.7%.
Passive treatments such as acupuncture, massage therapy, and stimulation can sometimes be used as a complement to active exercise. Returning to normal activities of everyday life should be encouraged as soon as possible to maximize and accelerate full recovery.
For chronic whiplash patients, rehabilitation is recommended. Patients entering the rehabilitation program say they are able to control their pain, they continue to use the strategies taught to them, and can return to their daily activities.
Drugs
According to recommendations made by the Quebec Task Force, treatment for individuals with class 1-3 whiplash-related disorders may include non-narcotic analgesics. Non-steroidal anti-inflammatory drugs may also be prescribed in the case of WAD 2 and WAD 3, but their use should be limited to a maximum of three weeks. Botulinum toxin A is used to treat contractions and spontaneous muscle spasms. A-type botulinum toxin is only a temporary and repeated injection that needs to be done to feel the effect.
According to a one-year follow-up study in 2008 in 186 patients, the WAD-classification and Quebec Task Force regimens were not associated with better clinical outcomes.
Prognosis
The consequences of whiplash range from mild pain for several days (which is the case for most people), to severe disability. It seems that about 50% will have some symptoms left over.
Changes in cerebral blood flow resting conditions have been demonstrated in patients with chronic pain after a whiplash injury. There is evidence for permanent inflammation in the neck in patients with chronic pain after a whiplash injury.
There has long been a proposed relationship between whiplash injury and the development of temporomandibular joint dysfunction (TMD). A recent review concludes that although there are contradictions in the literature, there is overall moderate evidence that TMD can sometimes follow whiplash injuries, and that the incidence of these events is low to moderate.
Epidemiology
Whiplash is a term commonly used to describe hyperflection and hyperextension, and is one of the most common non-fatal car crash injuries. More than one million whiplash injuries occur each year due to car accidents. This is an estimate because not all cases of whiplash are reported. In certain years, an estimated 3.8 people per 1000 symptoms experience whiplash. "Freeman and fellow investigators estimate that 6.2% of the US population has late whiplash syndrome". The majority of cases occur in patients at the end of the fourth decade. Unless a cervical tension with brain death or spinal cord trauma is rare.
Whiplash can occur at speeds of fifteen miles per hour or less; it was a sudden jerk, when one car hit another, causing one's head to suddenly be thrown back and sideways. The more sudden the movement, the more bones, discs, muscles and tendons in the neck and upper back will be damaged. Spinal cord injuries are responsible for about 6,000 deaths in the US each year and 5,000 whiplash injuries per year resulting in quadriplegia.
After 12 months, only 1 in 5 patients remained symptomatic, only 11.5% of individuals were able to return to work a year after the injury, and only 35.4% were able to return to work at the same level of performance after 20 years. The indirect cost estimate for industry is $ 66,626 per year, depending on the level and severity. Finally, the total cost per year was $ 40.5 billion in 2008, a 317% increase over 1998.

References
External links
Source of the article : Wikipedia
